Soaking in some badly needed sunshine to boost my Vit D level, an important immune-boosting measure, on my way to badminton games.
Common sense and both western and Chinese medicine tell us that eating a healthy diet, exercise, and balanced nutrition is a major part of disease prevention measures, Covid-19 included.
The warm April southeastern US sunshine and breeze caressed my face when I drove to my badminton games, with the top down to absorb as much sunshine as possible, to boost vitamin D level to protect my health, to boost my immune system against viral infections, esp. SARS-Cov-2. I thought to myself.
In addition to Vit D, I have also been taking Vit C, zinc, quercetin, other vitamins, and antioxidants as part of my routine immune boosting and health maintenance measures. As a result, my health today is a lot better than 10 years ago.
I just received an invitation again as a guest on a TV network (CGTV, the English channel of China’s Central TV network) to talk about the integrative medical approach (traditional Chinese medicine) to Covid-19 (April 26th at 9:30 pm EST at CGTN.com/america/livenews). I have been a regular guest on their shows for over a year now. This is one of the few media outlets that I can share my views on medicine and health. I have been censored numerous times on other social media platforms for sharing my scientific research and patient management experience.
This (the integrative approach) is also part of the topics of my invited presentation at the 50th Annual Conference of the International Orthomolecular Medicine (https://isom.ca/event/50th-conference/): most people who catch the SARS-Cov-2 virus don’t develop diseases or at most have mild to moderate diseases. Only a very small percentage of those infected with SARS-Cov-2 develop clinically severe or critical diseases.
Why do some people develop serious diseases while most don’t? We all know that the elderly and people with chronic diseases tend to have higher mortality rates and more serious diseases of Covid-19. The bottom line is that it’s one’s health status that determines the outcome when one catches a pathogen. To prevent oneself from catching an infection, or to reduce the severity of an infection, one needs to boost his/her immunity. This is simply common sense. Do we really need to quote the abundantly available research data to support this conclusion?
While enjoying the ride and organizing my thoughts on my CGTV interview, I can’t shake off the disturbing email I just received. One of my friends sent me an email about the “Covid-19 Protection Act” and its first victim. It read:
And the first victim to suffer under this new law is a St. Louis chiropractor who was recommending Vitamin D and zinc supplements to his clients and is now charged as a criminal…
More lunacy from the federal government threatens doctors with $10,000 fines if they tell you the science about how vitamins and minerals can help with COVID. (https://healthimpactnews.com/2021/covid-natural-remedies-banned-as-doj-and-ftc-seek-to-silence-doctors-promoting-vitamin-d-c-zinc-etc/).
This morning, I also received a completed video from Dr. Susan Downs who interviewed me on my thoughts on censorship (https://vimeo.com/536631433). In this video, Susan and Kevin Sorbo interviewed many doctors (myself included), scientists, patients, and others on Big Media’s censorship. I remember the moment during the interview when I got a bit emotional because I simply couldn’t believe that this final “land of freedom”, my adopted country is rapidly looking more and more like the land where I escaped from 35 years ago.
Where else can I escape to?
Finished my badminton games, sweated, feeling relaxed, comfortable, and tired, I had a good night’s sleep. This morning, while I try to finish this short commentary, I read an email from one of my heroes, Dr. Joe Mercola whose article “Wake Up! COVID Is a Setup to Destroy Human Liberty” (https://articles.mercola.com/sites/articles/archive/2021/04/25/naomi-wolf-the-end-of-america.aspx) sent another chill down my spine. In Joe’s interview of Naomi Wolf, Wolf listed 10 steps towards tyranny and we are at Step 10.
We are rapidly approaching the “point of no return” towards tyranny.
So what’s going on in America?
Educating the public about living a healthy lifestyle with balanced and optimal nutritional support to boost our immune system to protect or prevent Covid-19 or other diseases becomes illegal and could be prosecuted?
Do we need RTC data to support Vit C, Vit D’s effect in Covid-19 protection and treatment, otherwise whoever promotes these will be prosecuted? Then what about a healthy lifestyle and exercise? If I educate and promote a healthy lifestyle, eat a healthy diet, and exercise to improve our health to prevent or reduce the severity of Covid-19, am I violating this “Covid-19 Consumer Protection Act”? I have not seen any clinical trials that are specifically designed for Covid-19. So without clinical trial data, we can’t tell our patients of these common-sense approaches? Otherwise, I may be prosecuted?
All of a sudden, I suddenly feel I don’t know how to practice medicine anymore, after 40+ years in medicine. Is this “Covid-19 Consumer Protection Act” really helping the consumers or hurting the consumers?
My medical career, along with my Ph.D. in biochemistry and my deeply rooted traditional Chinese medicine philosophy has taught me that to prevent diseases, to achieve optimal health and longevity, one needs to take an integrated approach of what I call “3 New View of Health/Medicine”, Integrative, Natural and Balanced views.
This is also going to be a topic of my CGTN interview and my ISOM presentation.
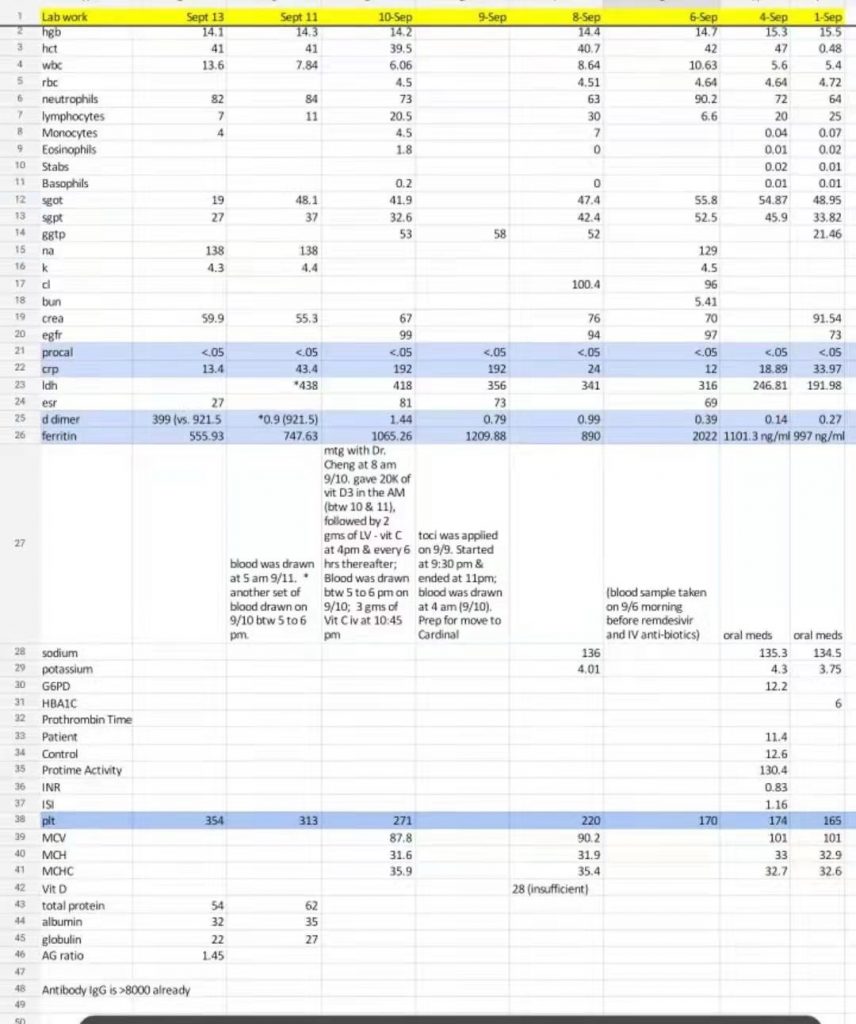
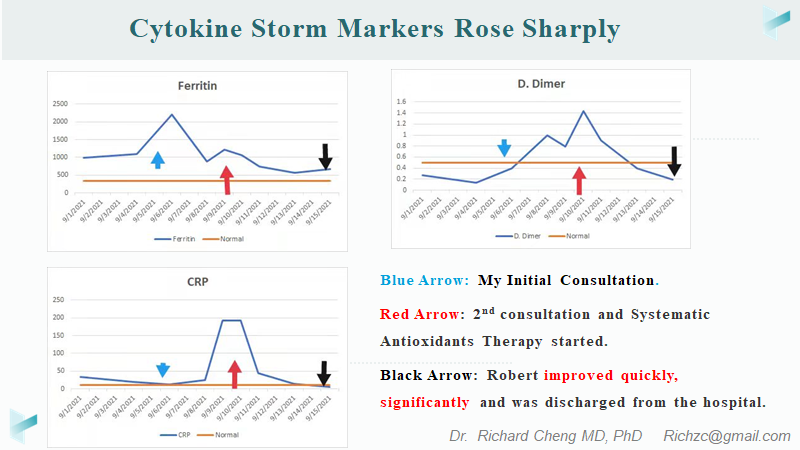
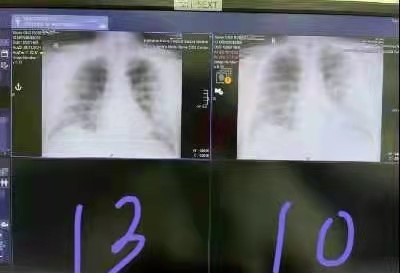
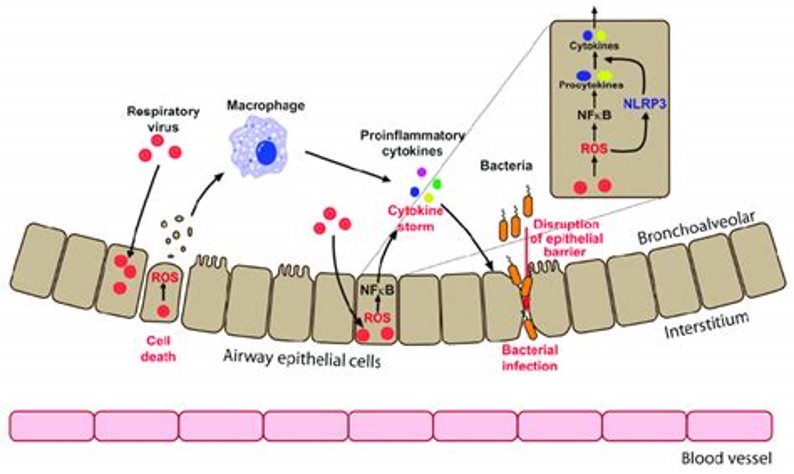
The focus of ISOM presentation is on the true understanding of Covid-19: the key mechanism leading to severe Covid-19 in the small number of patients is the cytokine storm/exuberant oxidative stress, which I (and others) pointed out over a year ago (https://pubmed.ncbi.nlm.nih.gov/32328576/).
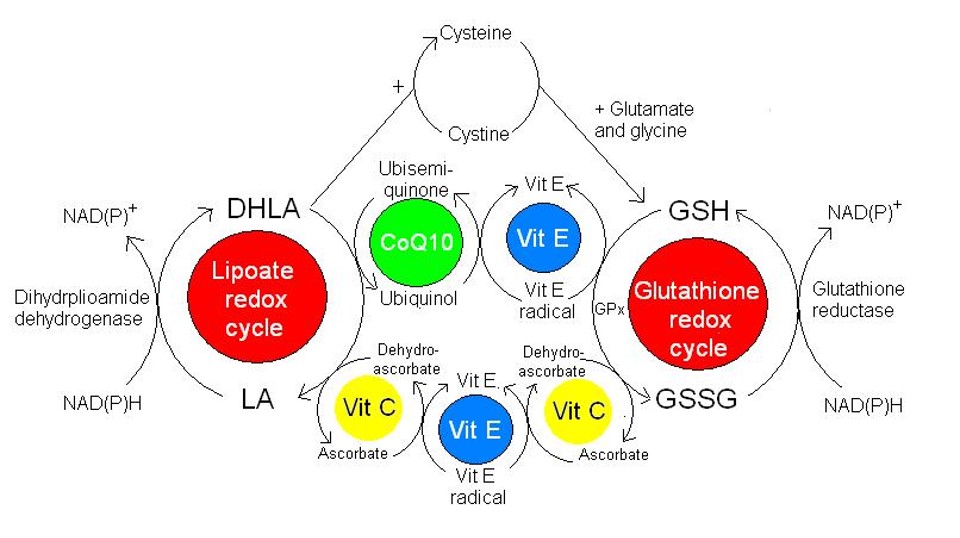
To prevent the cytokine storm/oxidative stress with early and sufficiently dosed antioxidants, esp. lipid membrane-associated antioxidants system(vitamins E, C, glutathione, lipoic acid, CoQ10, etc) will help to stabilize cell membranes and prevent lipid oxidation. There has been abundant basic research and clinical data to support this before the Covid-19 Pandemic. If this “antioxidant” approach was adopted as we (and others) proposed early in the pandemic, we may not be in the position we are in today. In a little over a year, more research (more than 2500 papers in Pubmed.gov to be specific) appeared on this topic, providing direct research and clinical data on Covid-19. What more do we need?
Antioxidants for prevention and treatment are Safe, Inexpensive, and Effective (with early and sufficient dosing). The benefit/risk ratio for patients clearly dictates the wide application of this approach. This approach is not only not widely used, but now the education/promotion/recommendation of this approach under the “Covid-19 Consumer Protection Act” is even illegal and may be prosecuted?
What world do we live in today?
I remember an old Chinese saying: 忍无可忍便不再忍 (If I can’t bear it, I won’t bear it anymore).
Richard Cheng, M.D., Ph.D.
4/26/2021